Case Study: Knee Arthroscopy: ACL Repair
with Medial Meniscectomy in a 32 year-old male
Meniscus removal from the outside of the knee is known as a partial lateral meniscectomy, and meniscus removal from the inside of the knee is known as a partial medial meniscectomy. A total meniscectomy is quite uncommon.
A 32 year-old male patient visits the office with right knee pain after having a fall in a volleyball game. The patient is active and had a fall on his right lower extremity with the pivoting injury while playing volleyball about two weeks back. He was seen in the office a couple of times. His knee was paining and buckling.
An MRI was done, which showed a tear of the ACL as well as medial meniscus. We discussed treatment options and the patient opted for surgical management. We discussed repair versus reconstruction of the ACL and repair versus meniscectomy of the medial meniscus.
We discussed risks and benefits including infection, bleeding, injury to adjacent nerves and vessels, failure and need for repeat surgery, rehabilitation, arthritis, systemic complications including blood clots, cardiac, pulmonary, neurologic complications including death. The patient understood and signed an informed consent.
The patient was taken to the operating room where he was placed on a well-padded operating table. General anesthesia was given. Preop, 2 g of Ancef and 1 g of TXA was given.
Right lower extremity was prepped and draped aseptically in the usual fashion after application of high-thigh tourniquet. The exsanguination of the right lower extremity was done and tourniquet was elevated.
Arthroscopy was made through the lateral parapatellar incision. Arthroscope was inserted. Examination of the medial and lateral meniscus use of spinal needle. The examination of the intercondylar notch showed rupture of the ACL at the proximal end.
Further examination showed that the ACI was reparable and the decision was made to repair the ACL. Examination of the lateral tibiofemoral compartment showed intact meniscus and intact cartilage. The medial meniscectomy was done with the use of shaver and biters.
The debridement of the medial wall of the lateral femoral condyle was done with the shaver in order to prepare for insertion of the ACL stump. Once the prep was done, tibial tendon was drilled with the use of ACL tibial jig and Fiber Stick was used to keep the tunnel patent.
Fiber links were used by x2 to pass superior through the anteromedial and posterolateral bundle of ACL with the use of Scorpion. The sutures were taken out through the separate incision.
Femoral tunnel was drilled with the use of the same drill and ACL femoral jig out from the lateral femoral condyle at the region of the ACL stump. Fiber Stick was then used. The Fiber Links were loaded with the Fiber Tape The button was passed from the femoral tunnel and flipped on the lateral cortex under the IT band.
Then pull the Fiber Tape inside the tunnel. The Fiber Links were also tightened to pull the ACL stump on to the left bundle. This was found to be reduced in a satisfactory position.
The tibial end of the Fiber Tape was passed through the tibial tunnel with the end tightened and the knee was cycled. The tibial end was fixed to the tibia with the use of 4.75 SwiveLock in extension. The knee was again cycled and tightened the femoral side and knotted to each other.
The ACI Fiber Links were also tightened after cycling the knee and knotted to each other. The sutures were cut with the use of blades. Final pictures were taken and saved. The knee was thoroughly irrigated and ranged.
Closure was done with the use of # 3-0 nylon. Dressing was done with the use of Xeroform, 4 x 8s, ABD, Webril and Ace wrap. Knee immobilizer was applied and locked in extension. The patient was extubated and moved to recovery in a stable condition. Postoperative adductor canal block was given by the anesthesia team.
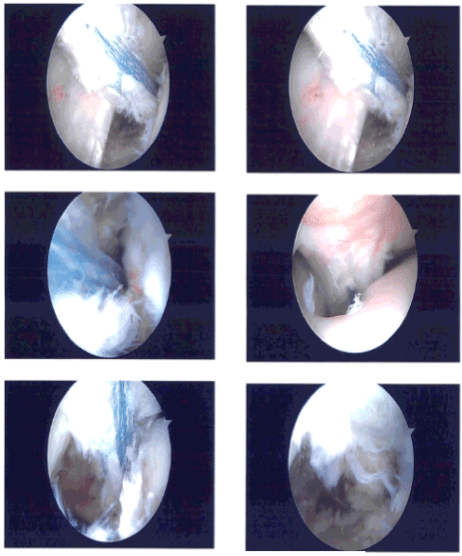
Clinical photo
After a week the patient went to the office for his post operative visits, no x-rays were needed. The patient has been having a rash on the knee as well as on thigh and leg and arm too. He denies chills and had about 99 F temp one night.
After discussing treatment options, we have decided to proceed with formal physical therapy as well as a home exercise program for rehabilitation of the knee. We went over the arthroscopic pictures and removed the stitches during the visits.
We will continue with ice and elevation of the knee to decrease swelling and pain. We will continue to utilize early mobilization and mechanical prophylaxis to reduce the chances of a deep vein thrombosis. We will wean them off any narcotic medications and progress to anti-inflammatories and Tylenol as long as there are no contraindications to these medications.
We also discussed the risk and benefits and common side effects of taking these medications. He is to see his PCP for a rash. We talked and he added antibiotics to cover for MRSA. He had been having a rash and swelling on the knee as well as on thigh and leg and arm too.
He was treated with antibiotics and cream. He got his blood work last week and then repeated CRP yesterday which has not been reported. Previous CRP was 35 with mild neutrophilia and leukocytosis. He is being seen by his PCP also.
After 2 weeks the patient was here again for his postoperative visit, no x rays were needed. His CRP had decreased to 11, 2 weeks back. His rash has resolved. He has no fever, chills, pain, swelling, redness. He is using bledsoe and no crutches. The patient is improving and needs to strengthen the Quads.
He is continuing with Physical Therapy and hamstrings and Home therapy, Back therapy. After the operation, the patient recovered well and kept up with physical therapy. After a month, the patient returned for a follow-up visit and his knee had much improved.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.

I am Vedant Vaksha, Fellowship trained Spine, Sports and Arthroscopic Surgeon at Complete Orthopedics. I take care of patients with ailments of the neck, back, shoulder, knee, elbow and ankle. I personally approve this content and have written most of it myself.
Please take a look at my profile page and don't hesitate to come in and talk.